


Fascia & Self-Massage7 min read
Fascia Research: What Science Knows About Fascia
published by Prof. Dr. Robert Schleip in Fascia & Self-Massage on 14/04/2021 - updated at 23/06/2026

Prof. Dr. Robert Schleip
01. When Was Fascia Discovered? – The History of Fascia
The first article published in the medical database PubMed that included the term “fascia” dates back to 1814. Even then, it was noted that fascia separates muscles and supports movement (Mackesy 1814). To this day, this view has not changed, even though countless studies on fascia have been conducted since then.
However, thanks to this new knowledge, our understanding of fascia has expanded significantly, leading to several changes in its definition. This is particularly true for the last four decades. As fascia research continues to advance, the description of fascia will continue to evolve. (Adstrum and Nicholson 2019)
In a recent update to fascial nomenclature, the definition of fascia is somewhat abbreviated and, loosely translated, reads: “Any tissue capable of responding to mechanical stimuli can be referred to as fascia.” The three-dimensional fascial continuum arises from a perfect synergy between various tissues—including all their solids and fluids—that permeate, divide, connect, and nourish the entire body, from the superficial layer of skin down to the bone.
These include, for example, muscle and nerve sheaths, joint capsules, ligaments, tendons, as well as blood and lymph vessels with the fluids circulating within them” (Stecco, Carla et al., “Update on Fascial Nomenclature,” Journal of Bodywork and Movement Therapies, Volume 22, Issue 2, 354).
In-depth research on fascia has now been ongoing for more than three decades. Here, we provide you with an overview of the most important scientific findings and studies on fascia.
02. Anatomy of Fascia
The Three Layers of Fascia
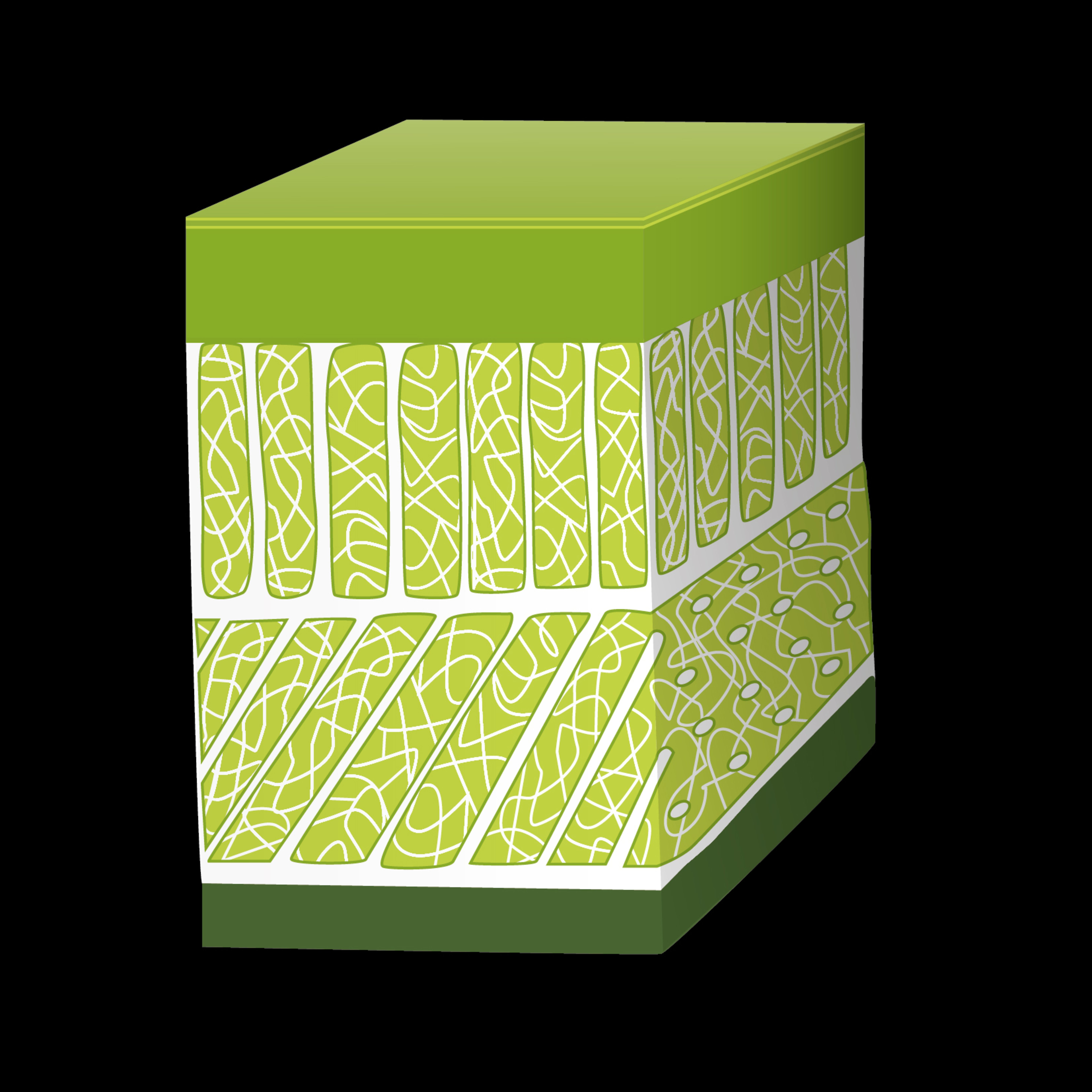
Fascia consists of three distinct layers: the superficial, deep, and parietal/visceral layers (Gatt et al. 2020).
The superficial layer of fascia contains many elastic fibers, making it quite mobile. In contrast, the deep layer, due to its high proportion of collagen fibers, is significantly firmer and exhibits a certain degree of constant tension.
For example, it is responsible for transmitting forces generated by muscles to neighboring regions. Within these regions, proprioceptors are stimulated, among other things, and the information they provide is important for body awareness and movement (Klingler et al. 2014).
Contractility of the Fascia
The notion that fascia plays an exclusively passive role in force transmission has been unequivocally refuted in recent years by several medical studies. Fascia contains contractile elements, known as myofibroblasts, which contribute to force generation and can modulate it.
In addition, they contribute to a certain degree of mechanosensory fine-tuning, allowing information from the body to be processed more sensitively. Unlike muscles, however, fascia contract autonomously (e.g., like the heart muscle). This means that the contraction is not under voluntary control.
Through their ability to contract, fascia can spontaneously regulate their stiffness and thus actively contribute to joint stabilization and dynamic movements over a period ranging from minutes to hours. If this regulatory mechanism becomes dysfunctional, myofascial tension increases or decreases, and/or neuromuscular coordination is impaired.
Both can contribute to the development of various musculoskeletal complaints and pain syndromes. It is believed that an increase in tension lasting from days to months can even lead to serious tissue contractures (Schleip and Klingler 2019; Klingler et al. 2014).
03. Fascia Models
Our understanding and explanation of how fascia functions in the human body has also evolved over the past few years. Three models are currently being discussed in fascia research: the biotensegrity model, the fascintegrity model, and the myofascial chain model (Bordoni et al. 2019; Bordoni et al. 2018).
Biotensegrity Model
The biotensegrity model was initially characterized by the term “tensegrity model.” Tensegrity refers to a mechanical equilibrium of tension within a structure and originates from architecture (Figures 1 and 2). From this, the biotensegrity model emerged to apply the understanding of a structure’s mechanical equilibrium of tension to the living body (Figure 3).
This model explains the body’s continuous adaptability, encompassing all its structures, without compromising their forms and functions. However, these mechanical models do not account for bodily fluids, which also contribute to mechanical tension and thereby determine the body’s form and function.

2) Tensegrity Model of the Spine: The spine is stabilized, among other things, by the tension of the ligaments and tendons. Image from: (Bordoni et al. 2018)

(3) Biotensegrity model of the fascial continuum in the human body. This image shows a seated man in perfect balance. It reflects the tensegrity model. Image from: (Bordoni et al. 2018)
Fascintegrative Model
This is why the Fascintegrative Model was developed. In addition to the solid components of connective tissue, which are taken into account in the Biotensegrity Model, this model includes bodily fluids. These include blood and lymph, as well as fluids inside and outside cells. This more accurately reflects the current state of knowledge regarding the fascial continuum.
Nevertheless, this model lacks, among other things, consideration of the emotional level and pain, which can influence the body and the fascial system just as strongly. Therefore, further explanatory models will certainly emerge from research in the future.
Myofascial Chains
Myofascial chains are described as pathways of muscles and fascia that run throughout the entire body and can transmit tension from one region of the body to other nearby or distant regions.
Although studies have shown that muscles are interconnected and that force is transmitted between them, the existence of frequently described myofascial chains has only been partially scientifically proven. In particular, their functional relevance is not yet fully understood.
However, there is evidence that disruptions in myofascial connections may contribute to the development of musculoskeletal complaints and that treating these disruptions may help counteract them (Ajimsha et al. 2020; Wilke and Krause 2019; Krause et al. 2016; Wilke et al. 2016).
All of the models described depict the human body as a fascial continuum. They are used to explain this continuum. To date, however, they can only be considered theoretical models, as empirical evidence and scientific proof in living humans are lacking in many respects. Further research on fascia is needed to fully understand the complexity of the fascial system and how it functions (Bordoni et al. 2019).
04. Fascia in Connection with (Back) Pain
Fascia can be responsible for pain. This has been demonstrated, for example, in the large fascia in the back region (fascia thoracolumbalis). It contains many nociceptive free nerve endings that can be irritated by micro-injuries or inflammation, which can subsequently trigger a perception of pain in the brain (Wilke et al. 2017).
These findings can, in turn, be applied to pain associated with muscle soreness or a muscle fiber tear. Muscle soreness involves small tears in the muscle fascia (Gibson et al. 2009), and a muscle fiber tear is typically a myofascial or myotendinous lesion (Wilke et al. 2019).
However, the nerve endings mentioned can also be irritated by pathologically altered fascia. Such fascia is often thicker and exhibits increased stiffness as well as reduced gliding ability. This is caused by fibrosis and adhesions within the fascial layers, which can result from a permanently altered posture and non-physiological movement patterns (Langevin et al. 2009; Klingler et al. 2014; Pavan et al. 2014).
This was recently demonstrated in participants with nonspecific back pain (Almeida et al. 2020). The altered large dorsal fascia in these participants also led to restricted mobility of the spine, as is commonly observed in many people with back problems. Flexion and rotation were particularly affected.
What can help?
Fascia training, as several studies have now shown. The most common studies published focus on the use of foam rollers and report the following findings: Foam rolling alters the flow properties of the fluid within the fascia, improves blood circulation, and increases water absorption in the fascia. This changes the stiffness and glideability of the fascia.
In addition, training with a foam roller has been shown to reduce pain and improve mobility. Although the reasons for this are not yet fully understood, it is likely that foam rolling activates mechanoreceptors in the skin and fascia, which in turn activate a central pain-inhibiting mechanism, regulate the activity of the sympathetic and parasympathetic nervous systems (autonomic nervous system), and influence myofascial tension via a reflex response.
However, the common assumption that foam rolling therapy primarily serves to release adhesions in the fascia has not yet been proven (Guzmán-Pavón et al. 2020; Rodríguez-Fuentes et al. 2020; Behm and Wilke 2019; Wilke et al. 2018).
05. Conclusion on Fascia Research
Even though much has been learned about fascia in recent years through fascia research—including work by Dr. Robert Schleip, who is based at the University of Ulm—there is at least as much, if not more, that remains unknown. However, current knowledge is increasingly being integrated, leading to a continuously growing understanding of fascia and the effects of fascia training. It would be fascinating to look into the crystal ball. Research on fascia will certainly continue.




